BAXFENDY approved in the US as the first and only aldosterone synthase inhibitor treatment for adults with hypertension
BAXFENDY approved in the US as the first and only aldosterone synthase inhibitor treatment for adults with hypertension
Approval based on BaxHTN Phase III results showing statistically significant and clinically meaningful reduction in systolic blood pressure in patients with uncontrolled or resistant hypertension
BAXFENDY 2mg lowered systolic blood pressure by 15.7 mmHg (9.8 mmHg placebo-adjusted) from baseline in BaxHTN trial

WILMINGTON, Del.--(BUSINESS WIRE)--AstraZeneca’s BAXFENDY™ (baxdrostat) has been approved in the US as a first-in-class aldosterone synthase inhibitor (ASI) for the treatment of hypertension in combination with other antihypertensive medications, to lower blood pressure in adults who are not adequately controlled.
There are 1.4 billion people worldwide living with hypertension.1 In the US, approximately 50% of patients living with hypertension who are already taking multiple antihypertensive medications still struggle with persistently elevated blood pressure,2 which is a leading risk factor for cardiovascular disease and premature death.3,4 Hypertension is the most prevalent and significant modifiable cardiovascular risk factor worldwide, accounting for more deaths and disability than any other modifiable risk.5-7
BAXFENDY is a first-in-class, highly selective and potent ASI designed to lower blood pressure in a new way by specifically inhibiting the production of aldosterone,8 a hormone that raises blood pressure to unhealthy levels and increases the risk of heart and kidney problems.9-11
The approval by the US Food and Drug Administration (FDA) was based on positive results from the BaxHTN Phase III trial,12 with BAXFENDY demonstrating statistically significant and clinically meaningful seated systolic blood pressure reduction at both 2mg and 1mg doses in patients with uncontrolled and resistant hypertension on two or more medications. BAXFENDY was generally well-tolerated with no unanticipated safety findings.
Dr. Bryan Williams, Chair of Medicine at University College London, and BaxHTN primary investigator, said: “We have been waiting for an innovative medication like BAXFENDY for hypertension for many years. Its novel way of lowering blood pressure has the potential to transform clinical practice by targeting a root cause of persistently uncontrolled hypertension. In addition, the nearly double-digit placebo-adjusted systolic blood pressure reduction achieved with BAXFENDY is exciting and clinically meaningful for clinicians and patients. Epidemiological data indicate that a 10 mmHg decrease in systolic blood pressure is associated with a roughly 20% lower risk of serious cardiovascular events.”
John M. Clymer, Executive Director, National Forum for Heart Disease & Stroke Prevention, said: “Hypertension remains a staggeringly widespread silent killer and a leading risk factor for stroke, heart attack, kidney damage and dementia. Tens of millions of people struggle to control their blood pressure despite lifestyle changes and currently available treatments. Innovative, new treatments could help millions protect their heart, kidney and brain health.”
Ruud Dobber, Executive Vice President, BioPharmaceuticals Business Unit, AstraZeneca, said: “The approval of BAXFENDY offers a much‑needed, first-in-class innovation for people living with persistently uncontrolled hypertension who have not responded to or tolerated existing medicines. In the US, about 23 million patients are uncontrolled despite being on two or more medicines for hypertension, which is a disease that has seen little therapeutic progress for the past two decades.”
In the BaxHTN Phase III trial,13 published in the New England Journal of Medicine,12 BAXFENDY (baxdrostat) demonstrated statistically significant and clinically meaningful efficacy for the treatment of patients with hypertension on top of standard of care. At week 12, the absolute reduction from baseline in mean seated SBP was 15.7 mmHg (95% confidence interval [CI], -17.6 to -13.7) and placebo-adjusted reduction was 9.8 mmHg (95% CI, -12.6 to -7.0; p<0.001) for the 2mg dose. For the 1mg dose, the absolute reduction from baseline was 14.5 mmHg (95% CI, -16.5 to -12.5) and placebo-adjusted reduction was 8.7 mmHg (95% CI, -11.5 to -5.8; p<0.001). The reduction in mean seated SBP with placebo was 5.8 mmHg (95% CI, -7.9 to -3.8). Results were consistent across both uncontrolled and treatment-resistant subgroups.
IMPORTANT SAFETY INFORMATION for BAXFENDY™ (baxdrostat)
Warnings and Precautions
Hyperkalemia
BAXFENDY can cause hyperkalemia. Assess serum potassium prior to initiation of BAXFENDY and monitor periodically during treatment. Correct serum potassium abnormalities prior to initiation. More frequent monitoring is recommended for patients at increased risk of hyperkalemia (eg, patients ≥65 years of age, those with diabetes mellitus or chronic kidney disease, and those receiving concomitant medications that increase serum potassium). If hyperkalemia occurs, treat hyperkalemia and consider interrupting or discontinuing BAXFENDY. Consider more frequent monitoring in patients who restart BAXFENDY after experiencing hyperkalemia. Permanently discontinue if clinically significant hyperkalemia recurs.
Hyponatremia
BAXFENDY can cause hyponatremia. Assess serum sodium prior to initiation and monitor periodically during treatment. Correct serum sodium abnormalities prior to initiation. More frequent monitoring is recommended for patients with low baseline serum sodium concentrations and those at risk for hyponatremia. If clinically significant hyponatremia occurs, treat the hyponatremia and consider interrupting or discontinuing BAXFENDY. Consider more frequent monitoring of serum sodium in patients who restart BAXFENDY after experiencing hyponatremia. Permanently discontinue if clinically significant hyponatremia recurs.
Adverse Reactions
Most frequently reported adverse reactions (≥2% with BAXFENDY and greater (≥1%) than placebo in pooled, placebo-controlled trials) reported for BAXFENDY 1 mg and 2 mg, respectively, were hyperkalemia (6.6%, 10.2%), hypotension (2.1%, 3.6%), hyponatremia (2.1%, 3.2%), dizziness (3.0%, 2.9%), and muscle spasms (1.8%, 2.9%).
Drug Interactions
Drugs That Increase Serum Potassium: Monitor serum potassium more frequently when BAXFENDY is used concomitantly with drugs that impair potassium secretion or increase serum potassium. Concomitant use may increase the risk of hyperkalemia.
Strong and moderate CYP3A inducers: Monitor the therapeutic effect of BAXFENDY more frequently during concomitant use. BAXFENDY is a CYP3A substrate.
INDICATION for BAXFENDY™ (baxdrostat)
BAXFENDY is an aldosterone synthase inhibitor indicated, in combination with other antihypertensive drugs, for the treatment of hypertension to lower blood pressure in adults who are not adequately controlled on other agents. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
Dosing
The recommended dosage of BAXFENDY is 2 mg orally once daily. For patients at increased risk of hyperkalemia or hyponatremia, the recommended dosage is 1 mg orally once daily.
Please see accompanying US Full Prescribing Information for BAXFENDY, including Patient Information.
You may report side effects related to AstraZeneca products.
Notes
Uncontrolled hypertension
Hypertension is a medical condition characterized by consistently high blood pressure levels, affecting an estimated 1.4 billion people worldwide.1,14,15 Over time, this can damage blood vessels and vital organs, increasing the risk of serious health problems such as heart attack, stroke, heart failure and kidney disease.14,15
Treated but uncontrolled patients with hypertension are at a significantly greater risk of all-cause mortality, heart-disease specific mortality, stroke-related mortality, CVD-specific mortality and dementia than patients whose hypertension is controlled. A large meta-analysis found that lowering systolic blood pressure by 10 mmHg can reduce the risk of major adverse cardiovascular events by around 20%,16 underscoring the urgent need for new treatments that target a key hypertension pathway at its source.
An observational study of nearly 60,000 patients studied over a median of 9.7 years showed that a 9.5 mmHg increase in SBP was associated with a 30% increase in risk of all-cause mortality and 41% increase in risk of cardiovascular death.17 Studies have shown that increased night-time blood pressure is associated with higher cardiovascular risk,18,19 and patients with hypertension have a higher risk of cardiovascular events like heart attack, stroke and death around the time of their morning blood pressure surge.20,21
Aldosterone, a hormone that raises blood pressure to unhealthy levels by promoting sodium and water retention9,10 is a key contributor to persistently uncontrolled hypertension. Elevated aldosterone levels, along with factors such as obesity, high salt intake, and various genetic or secondary conditions,22 are strongly associated with poor blood pressure control and the progression of heart failure and kidney disease. When left untreated, hypertension significantly increases the risk of cardiovascular and kidney-related complications.5,14,23
BaxHTN trial
The BaxHTN Phase III trial13 had three components to it that supported the following endpoints. The primary endpoint was assessed during a 12-week double-blind, placebo-controlled period. A total of 796 patients were characterized in a 1:1:1 ratio to receive BAXFENDY 2mg, 1mg or placebo once daily on top of standard of care [2 antihypertensive agents at baseline, one of which is a diuretic for uncontrolled hypertension and ≥ 3 antihypertensive agents at baseline, one of which is a diuretic for resistant hypertension]. The primary efficacy endpoint was the difference in mean change from baseline in seated SBP at week 12 between participants treated with baxdrostat (2mg or 1mg separately) and participants treated with placebo. Persistence of efficacy was assessed during a randomized withdrawal period from week 24 to week 32. Approximately 300 patients treated with BAXFENDY 2mg were re-randomized in a 2:1 ratio to either continue receiving baxdrostat 2mg or placebo for the 8 weeks. SBP at the end of the 8 weeks was compared with placebo and the BAXFENDY 2mg dose. Long-term safety was assessed at the end of the 52 weeks compared to a standard of care arm.
Additional confirmatory secondary endpoints include the effect of BAXFENDY versus placebo on seated SBP at week 12 in the resistant hypertension subpopulation, the effect of BAXFENDY versus placebo on seated diastolic blood pressure at week 12, and proportion of participants achieving seated SBP less than 130 mmHg at week 12.
BAXFENDY and the clinical development program
BAXFENDY is a first-in-class, highly selective and potent, oral, small molecule that inhibits aldosterone synthase,8 an enzyme encoded by the CYP11B2 gene, which is responsible for the synthesis of aldosterone in the adrenal gland.10 In clinical trials, BAXFENDY was observed to significantly lower aldosterone levels without affecting cortisol levels across a wide range of doses.24,25
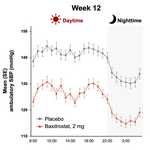
As part of a broad development program, BAXFENDY is currently being investigated in clinical trials in other conditions where high aldosterone plays a role in elevating cardiorenal risk, including as a monotherapy for primary aldosteronism,26 and in combination with dapagliflozin for chronic kidney disease and hypertension,27,28 and the prevention of heart failure in patients with hypertension.29 Additional clinical data for BAXFENDY in hypertension includes positive data from the Bax24 Phase III trial,30 which showed a statistically significant and highly clinically meaningful placebo-adjusted reduction of 24-hour ambulatory systolic blood pressure in patients with resistant hypertension, with full results published in The Lancet.31
AstraZeneca acquired BAXFENDY through its purchase of CinCor Pharma, Inc. in February 2023.32
AstraZeneca in CVRM
Cardiovascular, Renal and Metabolism (CVRM), part of BioPharmaceuticals, forms one of AstraZeneca’s main disease areas and is a key growth driver for the Company. By following the science to understand more clearly the underlying links between the heart, kidneys, liver and pancreas, AstraZeneca is investing in a portfolio of medicines for organ protection by slowing or stopping disease progression, and ultimately paving the way towards regenerative therapies. The Company’s ambition is to improve and save the lives of millions of people, by better understanding the interconnections between CVRM diseases and targeting the mechanisms that drive them, so we can detect, diagnose and treat people earlier and more effectively.
AstraZeneca
AstraZeneca (LSE/STO/NYSE: AZN) is a global, science-led biopharmaceutical company that focuses on the discovery, development, and commercialization of prescription medicines in Oncology, Rare Diseases, and BioPharmaceuticals, including Cardiovascular, Renal & Metabolism, and Respiratory & Immunology. Based in Cambridge, UK, AstraZeneca’s innovative medicines are sold in more than 125 countries and used by millions of patients worldwide. Please visit astrazeneca-us.com and follow the Company on social media @AstraZeneca. The contents of AstraZeneca’s website do not form part of this document and no one should rely on such websites or the contents thereof in reading this document.
References
- World Health Organization. Global report on hypertension 2025: high stakes: turning evidence into action. 2025. https://iris.who.int/handle/10665/382841. Accessed September 2025.
- Carey RM, et al. Prevalence of Apparent Treatment-Resistant Hypertension in the United States. Hypertension.2019;73(2):424-431.
- Rapsomaniki E, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet. 2014 May 31;383(9932):1899-911.
- GBD 2019 Risk Factors Collaborators. Lancet. 2020;396:1223-1249.
- Zhou D, et al. Uncontrolled hypertension increases risk of all-cause and cardiovascular disease mortality in US adults: the NHANES III Linked Mortality Study. Sci Rep. 2018: 20;8(1):9418.
- Hall ME et al. Weight-loss strategies for prevention and treatment of hypertension: a scientific statement from the American Heart Association. Hypertension. 2021;78:e38-e50.
- GBD 2023 Disease and Injury and Risk Factor Collaborators. Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 2025;406:1873-1922.
- Bogman K, et al. Preclinical and early clinical profile of a highly selective and potent oral inhibitor of aldosterone synthase (CYP11B2). Hypertension. 2017;69:189-96.
- Inoue K, et al. Serum aldosterone concentration, blood pressure, and coronary artery calcium: the Multi-Ethnic Study of Atherosclerosis [including online supplement]. Hypertension. 2020;76(1):113-120.
- Cannavo A, et al. Aldosterone and mineralocorticoid receptor system in cardiovascular physiology and pathophysiology. Oxid Med Cell Longev. 2018;2018:1204598.
- Xanthakis V, Vasan RS. Aldosterone and the risk of hypertension. Curr Hypertens Rep. 2013;15(2):102-107.
- Flack JM, et al. Efficacy and Safety of Baxdrostat in Uncontrolled and Resistant Hypertension. N Engl J Med. 2025. Aug 30:10.1056/NEJMoa2507109. doi: 10.1056/NEJMoa2507109.
- ClinicalTrials.gov. A Study to Investigate the Efficacy and Safety of Baxdrostat in Participants With Uncontrolled Hypertension on Two or More Medications Including Participants With Resistant Hypertension (BaxHTN). Available at: https://clinicaltrials.gov/study/NCT06034743. Accessed April 2026.
- McEvoy JW, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. EurHeart J. 2024;45(38):3912-4018.
- Whelton PK, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):1269-1324.
- Ettehad, D. et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis; Lancet 2016;387:957–67.
- Staplin N, et al. Relationship between clinic and ambulatory blood pressure and mortality: an observational cohort study in 59 124 patients. Lancet. 2023;401(10393):2041-2050.
- Narita K, et al. Nighttime Home Blood Pressure Is Associated With the Cardiovascular Disease Events Risk in Treatment-Resistant Hypertension. Hypertension. 2022;79(2):e18-e20
- Niiranen TJ, Mäki J, Puukka P, Karanko H, Jula AM. Office, home, and ambulatory blood pressures as predictors of cardiovascular risk. Hypertension. 2014 Aug;64(2):281-6.
- Renna NF, et al. Morning blood pressure surge as a predictor of cardiovascular events in patients with hypertension. Blood Press Monit. 2023;28(3):149-157
- Kario K et al. Morning hypertension: the strongest independent risk factor for stroke in elderly hypertensive patients. Hypertens Res. 2006;29(8):581-7.
- van Oort S, et al. Association of cardiovascular risk factors and lifestyle behaviors with hypertension: a mendelian randomization study. Hypertension. 2020;76(6):1971-1979.
- Jones DW, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2025;152:e114–e218.
- Freeman MW, et al. Results from a phase 1, randomized, double-blind, multiple ascending dose study characterizing the pharmacokinetics and demonstrating the safety and selectivity of the aldosterone synthase inhibitor baxdrostat in healthy volunteers. Hypertens Res. 2023;46(1):108-118.
- Freeman MW, et al. Phase 2 trial of baxdrostat for treatment-resistant hypertension. N Engl J Med. 2023;388(5):395-405.
- ClinicalTrials.gov. A Study to Assess Efficacy and Safety of Baxdrostat in Participants With Primary Aldosteronism (BaxPA). Available at: https://clinicaltrials.gov/study/NCT07007793. Accessed April 2026.
- ClinicalTrials.gov. A Phase III Study to Investigate the Efficacy and Safety of Baxdrostat in Combination With Dapagliflozin on CKD Progression in Participants With CKD and High Blood Pressure. Available at: https://clinicaltrials.gov/study/NCT06268873. Accessed April 2026.
- ClinicalTrials.gov. A Phase III Renal Outcomes and Cardiovascular Mortality Study to Investigate the Efficacy and Safety of Baxdrostat in Combination With Dapagliflozin in Participants With Chronic Kidney Disease and High Blood Pressure (BaxDuo-Pacific). Available at: https://clinicaltrials.gov/study/NCT06742723. Accessed April 2026.
- ClinicalTrials.gov. Phase III Study Investigating Heart Failure and Cardiovascular Death With Baxdrostat in Combination With Dapagliflozin (Prevent-HF). Available at: https://clinicaltrials.gov/study/NCT06677060. Accessed April 2026.
- ClinicalTrials.gov. A Study to Investigate the Effect of Baxdrostat on Ambulatory Blood Pressure in Participants With Resistant Hypertension (Bax24). Available at: https://clinicaltrials.gov/study/NCT06168409. Accessed April 2026.
- Azizi M, Bax24 investigators, et al. Effect of baxdrostat on ambulatory blood pressure in patients with resistant hypertension (Bax24): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet. 2026 Mar 7;407(10532):988-999.
- AstraZeneca 2023. Acquisition of CinCor Pharma complete. Available at: https://www.astrazeneca.com/media-centre/press-releases/2023/astrazeneca-acquires-cincor-for-cardiorenal-asset.html. Accessed April 2026.
Contacts
Media Inquiries
Lauren-Jei McCarthy laurenjei.mccarthy@astrazeneca.com +1 347 918 7001
US Media Mailbox: usmediateam@astrazeneca.com