

Non-invasive Oxygen Therapies Delay or Prevent Intubation but Are Believed to Aerosolize Coronavirus by 80% of Global Physicians Treating COVID-19 in Hospitals
Non-invasive Oxygen Therapies Delay or Prevent Intubation but Are Believed to Aerosolize Coronavirus by 80% of Global Physicians Treating COVID-19 in Hospitals
34% of COVID-19 treating physicians still believe ventilators are used too rapidly according to their hospital protocols
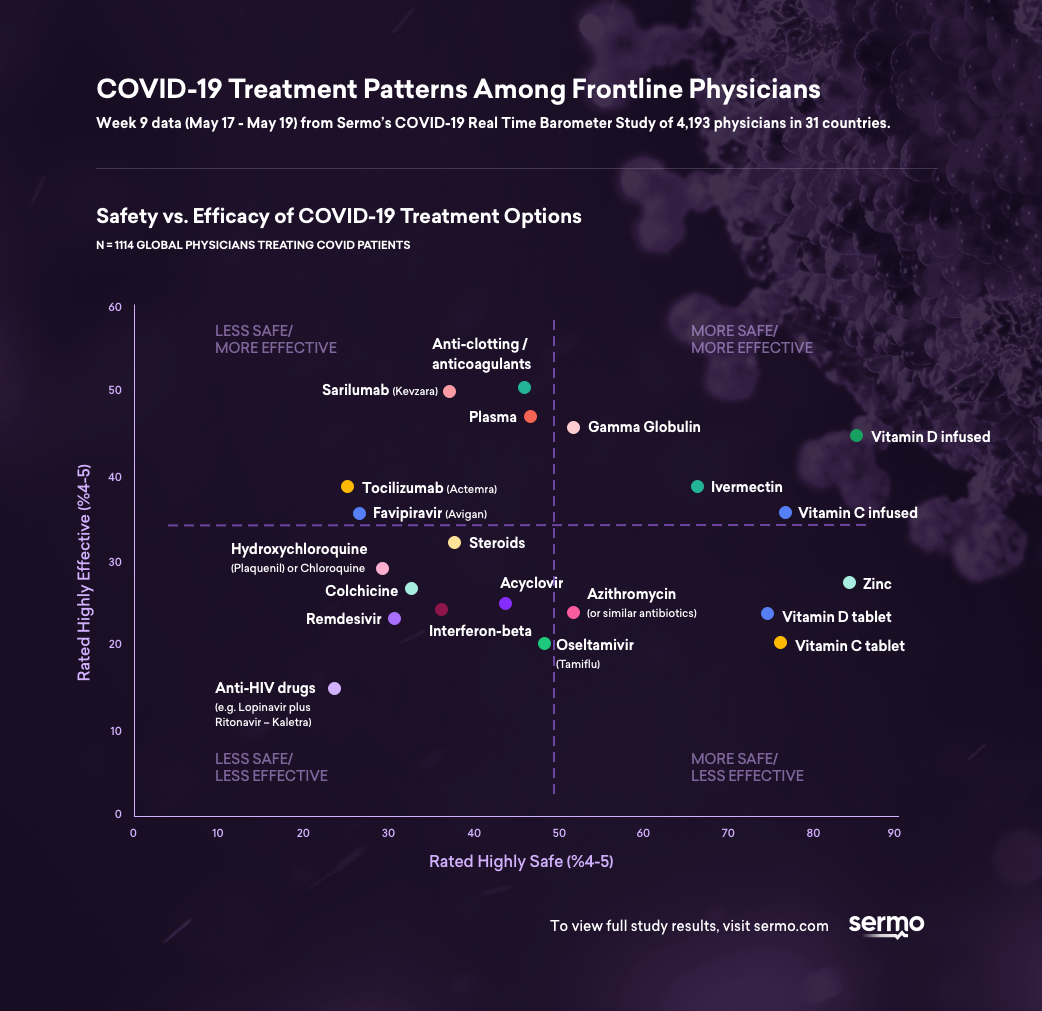
NEW YORK--(BUSINESS WIRE)--Week 9 (May 17 to 19) results from Sermo’s COVID-19 Real Time Barometer with 4,193 physicians reveal COVID-19 treatment patterns among frontline physicians. In total, Sermo’s Barometer study includes over 49,000 survey interviews in 31 countries, including the United States, Canada, United Kingdom, France, Brazil, Russia, China, Japan and Australia. Complete data published to date and study methodology can be found here.
Universal medical guidelines on COVID-19 and ventilation strategies have not been written or widely adopted yet. Despite the learning that early intubation was often unnecessary and potentially lethal to patients (with ventilator-related mortality rates documented up to 88%)1, many hospitals still have not changed their protocols. One possible reason is that the overwhelming majority of physicians believe non-invasive oxygen therapies put hospital staff and other patients at risk by aerosolizing the virus.
Initially, physicians treated COVID-19 as they would any other virus-induced pneumonia. Patients quickly developed breathing difficulties, treatment protocols were created on the fly, and rapid intubation was encouraged based on older guidelines. Panicked, governments purchased a surplus of very expensive ventilators and the U.S. president invoked the Defense Production Act to compel automotive companies to manufacture ventilators.
- This week (week 9) in Sermo’s COVID-19 Real Time Barometer, 72% of all doctors (base= 4193) and 80% of hospital physicians treating COVID-19 (base= 764) believe non-invasive ventilation aerosolizes the virus and increases the risk of infection to themselves, other healthcare professionals and patients.
Non-invasive oxygenation devices are inexpensive and widely available. They include heated high flow oxygen delivered via a face mask or nasal cannulas, sleep apnea machines such as continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BiPAP). CPAPs and BiPAPs work via a tube into a face mask, as opposed to invasive ventilation, which includes a tube placed deep in a patient’s throat while they are sedated, posing a much higher risk to the patient.
“At the outset of the pandemic, there were worldwide concerns about a shortage of ventilators. Non-invasive oxygen therapies, like CPAP and BiPAPs were and still are associated with an increased risk of virus transmission, and therefore many hospitals are still moving directly to invasive ventilation. If properly protected, physicians shouldn’t fear using these devices and should absolutely delay ventilation," said Dr. Mark Rumbak, Professor of Medicine, Pulmonary, Critical Care and Sleep Medicine, University of South Florida.
According to a recent study, non-invasive ventilation techniques were proven to be droplet (not aerosol)-generating procedures, producing droplets of > 10 µm in size. Due to their large mass, most fall onto local surfaces within 1 meter.
Gradually, the medical community began to see marked differences in the pathophysiology of the disease versus other known virus pneumonias, and in patient response. Physicians made a startling observation; many COVID-19 patients had blood oxygen levels so low they should have been either dead, gasping for air, or experiencing racing heartbeats from the lack of oxygen. Eventually, the medical community learned patients could tolerate these lower levels of oxygen.
“Oxygen blood levels have typically driven decisions about breathing support and intubation, but with COVID-19 they might be misleading. Additionally, many physicians are realizing respiratory failure of COVID-19 should be treated differently from routine Acute Respiratory Distress Syndrome (ARDS). It’s imperative to communicate that more patients could receive simpler, noninvasive oxygen support. These strategies should be used in the beginning of breathing difficulties and can even be used for the duration of the illness,” said Dr. Rumbak.
However, many physicians feel ventilators are still being used too quickly by their hospitals.
- In a May 4 Sermo survey, 47% of COVID-19 treating physicians agreed, “we are currently using ventilators too rapidly on patients and we should delay their use as much as possible trying all forms of oxygen therapy initially.” (N=1100 Covid treaters).
In this study, physicians also disagreed about whether they were seeing typical ARDS or a new phenomenon. In week 9 of the Barometer, the number of physicians believing ventilation was occurring too rapidly dropped to 34%, indicating intubations were being slowed down, but were still significantly “too rapid.”
Recently, several leading medical organizations have recommended delaying intubation and using non-invasive ventilation first. The NIH issued new guidelines advocating a phased approach to breathing support that defers the use of ventilators.
The Shanghai guidelines and The Lancet also recommend a similar approach, however, hospitals around the world are not adopting these strategies universally or quickly enough, and each hospital can decide themselves how to treat COVID-19 respiratory failure.
About the Real Time Barometer
The Real Time Barometer is an observational study of the impact of the COVID-19 outbreak as reported by physicians with firsthand experience of treating COVID-19 patients. Each week, thousands of physicians provide insights on topics regarding the global health crisis. To date, more than 49,000 doctors in 31 countries, including the United States, Canada, United Kingdom, France, Brazil, Russia, China, Japan and Australia have participated in the Barometer.
About Sermo
Sermo is the largest healthcare data collection company and social platform for physicians, reaching 1,3MM healthcare professionals across 150 countries. The platform enables doctors to anonymously talk real-world medicine, review treatment options via our proprietary Drug Ratings platform, collectively solve patient cases, and participate in medical market research. For more information, visit sermo.com.
Contacts
Media:
Angela Crawford
201-417-9157
Azito35@gmail.com


