
")
")
COPENHAGEN, Denmark--(BUSINESS WIRE)--For media outside China, Japan, UK, USA only.
Lundbeck today presented results at the American Psychiatric Association (APA) Congress from post hoc analyses in bipolar I disorder patients, which confirm that depressive symptoms are frequent during manic episodes.1
The post-hoc analyses also evaluated the efficacy of asenapine or placebo treatment (olanzapine active control) on manic and depressive symptoms in bipolar I disorder patients suffering manic episodes with mixed features as defined in DSM-5 (Diagnostic and Statistical Manual of Mental Disorders).
The analyses show that the more severe depressive symptoms are at baseline, the less likely patients will achieve remission (MADRS<=12).1 With increasing baseline severity of depressive symptoms, the post hoc analysis showed that treatment effect remained stable with asenapine but decreased with placebo.1
“We know from the scientific literature that many people with bipolar I disorder will experience depressive symptoms during a period of mania. Using the new DSM-5 criteria, a post hoc analysis confirms that depressive symptoms are frequent in these patients and generally remission rates of depressive symptoms decrease with increasing baseline severity,” said Dr Roger S McIntyre, Professor of Psychiatry and Pharmacology at the University of Toronto. “However, the post hoc analyses showed that asenapine efficacy was not affected by baseline severity of depressive symptoms meaning that the likelihood that patients achieve remission from depressive symptoms was stable across severity groups, unlike with placebo”.
Post-hoc analyses were conducted on pooled data from two identically designed 3-week, randomised, double-blind, flexible dose, placebo- and olanzapine-controlled trials. Analyses mirrored the DSM-5 definition of depressive symptoms during a manic episode by linking to the corresponding Montgomery-Åsberg Depression Rating Scale (MADRS) and Positive and Negative Syndrome Scale (PANSS) items. Patients were placed into three groups according to the number and severity of their depressive symptoms.1
Of the 960 patients included in the trials, just over half (56%) had three or more depressive symptoms at baseline. Of these, 34.2% were classified as mild, 17.5% as moderate and 4.3% as severe.1 The results of the post hoc analyses showed that an increase in the severity of depressive symptoms during mania was associated with poorer outcomes. In asenapine-treated patients, the remission rate of depressive symptoms during mania was stable regardless of symptoms severity (64-67%), and was statistically significantly superior (p≤0.05) vs placebo (49-25%) across all severity sub groups. The efficacy of asenapine on depressive symptoms was seen as early as week one of treatment.1
In addition, treatment with asenapine led to a significant reduction of manic symptoms in patients across all three subgroups of baseline depression severity.1
“Better understanding of the symptoms experienced by patients with bipolar I disorder is of utmost importance. Patients who experience mania with depressive symptoms and depression with manic symptoms are common and are associated with poorer treatment outcomes,” said Paul Arteel, Executive Director of GAMIAN Europe (Global Alliance of Mental Illness Advocacy Networks-Europe). “GAMIAN welcomes any research which can lead to improved management of bipolar I disorder for patients.”
Bipolar disorder affects 30 million people worldwide including over four million people in Europe.2 It is the sixth leading cause of disability worldwide.3 People with bipolar disorder are part of a medically-burdened population that often experience multiple complications.
Editor notes
About the post hoc analyses
The frequency of patients meeting the DSM-5 definition of manic episodes with mixed features among adults with bipolar I disorder was assessed in two randomized, double-blind, placebo–controlled asenapine studies. Patients included in these studies were included using the DSM-IV-TR definition. A further aim of the post hoc analyses was to determine the moderational effect of depressive symptoms on manic symptom reduction in adults with bipolar mania.1
The trials included patients with a DSM-IV-TR diagnosis of manic or mixed episode, as part of bipolar I disorder with a Young Mania Rating Scale (YMRS) total score ≥20 at baseline. This post hoc analysis mirrored the DSM-5 definition of manic episodes with mixed features by linking to corresponding MADRS/PANSS items. These definitions include depressed mood (MADRS item 1 or 2), diminished interest/pleasure (MADRS item 8), psychomotor retardation (PANSS item G7), fatigue, loss of energy (MADRS item 7), worthlessness, guilt feelings (MADRS item 9) and thoughts of death (MADRS item 10).1
Different severity cut-offs on MADRS/PANSS item scores were used to define depressive symptoms severity: mild: score ≥1 on MADRS items (≥2 for PANSS item); moderate: score ≥2 on MADRS items (≥3 for PANSS); and severe: score ≥3 on MADRS items (≥4 for PANSS). 1
About DSM-5
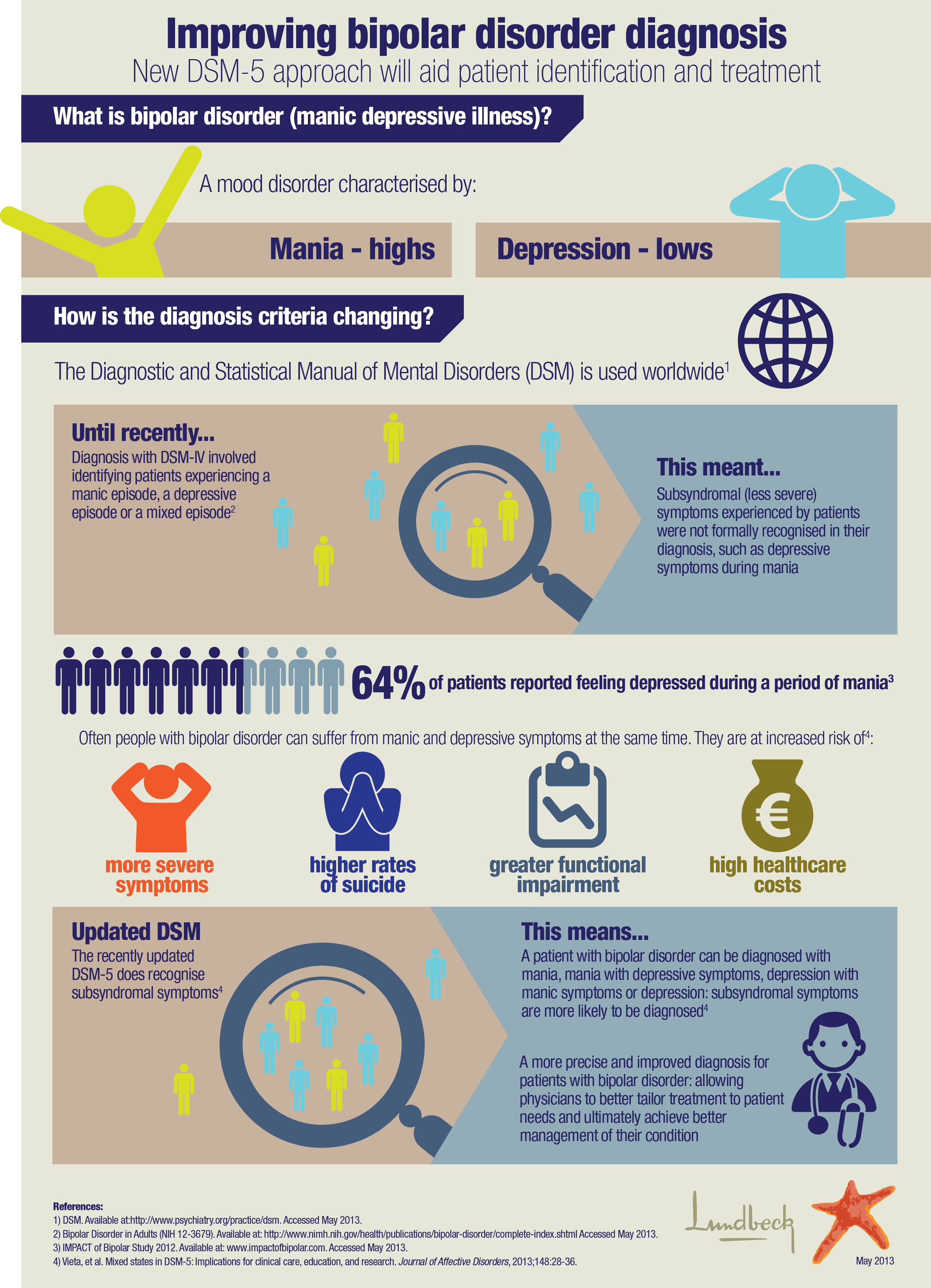
The Diagnostic and Statistical Manual of Mental Disorders (DSM) is a standard classification of mental disorders used worldwide by professionals in both clinical settings and community populations as a diagnosis and classification tool. It is also used as a tool for collecting and communicating accurate public health statistics about the diagnosis of psychiatric disorders.
The manual has been periodically reviewed and significantly revised since the publication of the first edition. DSM-5 is an update of the DSM-IV-TR edition and contains revised diagnostic criteria based on a comprehensive review of scientific advancements, targeted research analyses, and clinical expertise.
About bipolar I disorder
Bipolar I disorder (also known as manic-depressive disorder) is a chronic illness characterised by periods of mania (episodes of elevated moods, extreme irritability, decreased sleep and increased energy), depression (overwhelming feelings of sadness, suicidal thoughts), or a combination of both.4
About asenapine
Asenapine is the first tetracyclic antipsychotic with a different receptor profile. Asenapine is a sublingual tablet indicated for the treatment of moderate to severe manic episodes of bipolar I disorder in adults. Approximately 4,500 subjects, including more than 3,150 patients in phase II/III studies (including trials in schizophrenia), have contributed to asenapine safety and tolerability data and the clinical trial programme for asenapine has included nearly 1,300 patients with manic or mixed episodes of bipolar I disorder.5,6,7
About Lundbeck
H. Lundbeck A/S (LUN.CO, LUN DC, HLUKY) is an international pharmaceutical company highly committed to improving the quality of life for people suffering from brain disorders. For this purpose, Lundbeck is engaged in the research, development, production, marketing and sale of pharmaceuticals across the world. The company’s products are targeted at disorders such as depression and anxiety, psychotic disorders, epilepsy and Huntington’s, Alzheimer’s and Parkinson’s diseases.
Lundbeck was founded in 1915 by Hans Lundbeck in Copenhagen, Denmark. Today Lundbeck employs approximately 6,000 people worldwide. Lundbeck is one of the world’s leading pharmaceutical companies working with brain disorders. In 2011, the company's revenue was DKK 16.0 billion (approximately EUR 2.2 billion or USD 3.0 billion). For more information, please visit www.lundbeck.com.
References
1McIntyre, et al. DSM-5 Mixed Specifier for Manic Episodes: Evaluating the Effect of Depressive Features on Severity and Treatment Outcome Using Asenapine Clinical Trial Data. Presented at 166th Annual Meeting of the American Psychiatric Association (APA) May 2013.
2World Health Organization. Disease incidence, prevalence and disability. Available at: www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_part3.pdf. Accessed April 18, 2013.
3Kleinman, L et al. Costs of bipolar disorder. Pharmacoeconomics. 2003;21:601-622.
4National Institute of Mental Health. Bipolar Disorder 2009. Available at: www.nimh.nih.gov/health/publications/bipolar-disorder/nimh-bipolar-adults.pdf. Accessed August 24, 2012.
5Asenapine Summary of Product Characteristics, Feb. 2013.
6McIntyre, R et al. A 3-week, randomized, placebo-controlled trial of asenapine in the treatment of acute mania in bipolar mania and mixed states. Bipolar Disorders. 2009:11:673-686.
7McIntyre, R et al. Treatment of Mania in Bipolar I Disorder: Placebo and Olanzapine Controlled trials of Asenapine. Congress of European College of Neuropsychopharmacology, October 13-17, 2007, Vienna, Austria.