Newsroom
Sorted by: Latest
-
Se dan a conocer los diez finalistas del Reply AI Film Festival, el certamen internacional que aúna el cine y la inteligencia artificial
TURÍN, Italia--(BUSINESS WIRE)--El Reply AI Film Festival vuelve con su tercera edición, reafirmando su papel como punto de encuentro entre el cine, la creatividad y la inteligencia artificial. El concurso internacional creado por Reply, abierto a creativos que experimenten con nuevas tecnologías y herramientas de IA en la producción de cortometrajes, ha anunciado a sus diez finalistas. El festival tendrá lugar en Venecia durante los días en que se celebre la 83.ª edición del festival internaci...

-
Tien finalisten bekendgemaakt voor het Reply AI Film Festival, de internationale wedstrijd die film en kunstmatige intelligentie samenbrengt
TURIJN, Italië--(BUSINESS WIRE)--Het Reply AI Film Festival keert terug voor zijn derde editie en bevestigt daarmee opnieuw zijn rol als ontmoetingsplaats voor film, creativiteit en kunstmatige intelligentie. De internationale wedstrijd is opgericht door Reply en staat open voor creatieve makers die experimenteren met nieuwe AI-technologieën en -tools bij de productie van korte films. De tien finalisten zijn nu bekendgemaakt. Het festival vindt plaats in Venetië tijdens het 83e Internationale F...

-
Annonce des dix finalistes du Reply AI Film Festival, le concours international qui allie cinéma et intelligence artificielle
TURIN, Italie--(BUSINESS WIRE)--Le Reply AI Film Festival revient pour sa troisième édition, réaffirmant son rôle de point de rencontre entre le cinéma, la créativité et l’intelligence artificielle. Ce concours international créé par Reply, ouvert aux créatifs expérimentant de nouvelles technologies et de nouveaux outils d’IA dans la production de courts-métrages, a annoncé ses dix finalistes. Le festival se déroulera à Venise pendant la 83e édition du Festival international du film de Venise d...

-
Samenvatting: B-Secur en CSEM gaan samenwerken om klinisch gevalideerde hartbewaking naar wearables voor de gezondheidszorg te brengen
BELFAST, Noord-Ierland & NEUCHÂTEL, Zwitserland--(BUSINESS WIRE)--CSEM, het in Zwitserland gevestigde centrum voor technologische innovatie, en B-Secur, een toonaangevend bedrijf op het gebied van geavanceerde biosensortechnologie, hebben vandaag een samenwerking aangekondigd om klinisch gevalideerde hartbewaking mogelijk te maken in wearables voor de gezondheid. De samenwerking combineert de meer dan 25 jaar ervaring van CSEM op het gebied van bewaking van vitale functies via PPG (fotoplethysm...
-
B-Secur und CSEM integrieren klinisch validierte Herzüberwachung in Gesundheits-Wearables
BELFAST, Nordirland, und NEUCHÂTEL, Schweiz--(BUSINESS WIRE)--CSEM, ein Schweizer Technologie- und Innovationszentrum, und B-Secur, ein führender Anbieter fortschrittlicher Biosensorik, gaben heute eine Partnerschaft bekannt, um Gesundheits-Wearables mit klinisch validierten Funktionen zur Herzüberwachung auszustatten. Die Zusammenarbeit verbindet die mehr als 25-jährige Erfahrung und führende Stellung von CSEM in der PPG-basierten Überwachung von Vitalparametern mit den zahlreichen von der FDA...
-
First Internet Bank Puts AI-Powered Financial Intelligence Directly in Customers’ Hands
FISHERS, Ind.--(BUSINESS WIRE)--First Internet Bank today announced a secure new way for business and personal customers to unlock powerful, personalized financial insights from the accounts they already use every day. Through a permission-based connection to AI assistants such as OpenAI’s ChatGPT* and Anthropic’s Claude*, customers can ask questions in plain language and receive answers based on their own First Internet Bank account activity.The result is a breakthrough experience: financial an...
-
Attalon Advances U.S. Navy SONGBOW Program with $17.1 Million Office of Naval Research Award
PHILADELPHIA--(BUSINESS WIRE)--Attalon, a leading provider of advanced defense technologies, today announced it has received a $17.1 million contract modification from the Office of Naval Research under the SONGBOW program. The award supports the continued development of advanced pulsed fiber lasers and high-power directed energy subsystems for future U.S. Navy capabilities. Under the award, Attalon will continue developing pulsed fiber lasers for remote sensing and illumination while further m...
-
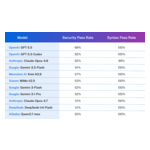
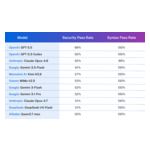
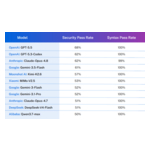
Los modelos de lenguaje grandes (LLM) son cada vez más inteligentes, pero no por eso más seguros: el informe "Veracode 2026 GenAI Code Security Report" revela que la seguridad del código generado por IA se ha estancado...
BURLINGTON, Mass.--(BUSINESS WIRE)-- Los modelos de lenguaje grandes (LLM) son cada vez más inteligentes, pero no por eso más seguros: el informe "Veracode 2026 GenAI Code Security Report" revela que la seguridad del código generado por IA se ha estancado en una tasa de aprobación del 56 % Veracode, líder mundial en gestión de riesgos de aplicaciones, publicó el día de hoy su 2026 GenAI Code Security Report (Informe sobre la seguridad del código de GenAI de 2026) que revela que, a pesar de los...
-
LLM's worden slimmer, maar niet veiliger: Veracode-rapport 'GenAI Code Security 2026' toont aan dat de veiligheid van door AI gegenereerde code stagneert op een slagingspercentage van 56%
BURLINGTON, Mass.--(BUSINESS WIRE)--Veracode, wereldwijd marktleider in risicobeheer voor applicaties, heeft vandaag het GenAI Code Security-rapport van 2026 uitgebracht. Hieruit blijkt dat de veiligheid stagneert, ondanks de snelle vooruitgang in de programmeercapaciteiten van AI. Op basis van vier meetmomenten en meer dan 100 modellen die sinds de start van het programma zijn gevolgd, ligt het gemiddelde slagingspercentage voor veiligheid op 56 procent – vrijwel ongewijzigd ten opzichte van h...
-
Les LLM gagnent en intelligence, mais pas en sécurité : le rapport 2026 de Veracode sur la sécurité du code généré par l'IA générative indique que la sécurité du code généré par l'IA stagne à un taux de réussite de 56 %
BURLINGTON, Massachusetts--(BUSINESS WIRE)--Veracode, leader mondial de la gestion des risques applicatifs, a publié aujourd'hui son rapport 2026 sur la sécurité du code GenAI. Celui-ci indique que la sécurité stagne, malgré les progrès rapides des capacités de codage IA. Sur quatre phases de test et plus de 100 modèles suivis depuis le début du programme, le taux de réussite moyen aux tests de sécurité s'établit à 56 %, un chiffre quasiment inchangé par rapport à l'année dernière. Chaque modèl...