

Newsroom
Sorted by: Latest
-
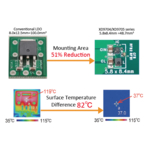
Torex Introduces Automotive AEC-Q100 Grade 1-Compliant 36V/600mA Compact Step-Down DC/DC Converter XD9704/XD9705 Series
TOKYO--(BUSINESS WIRE)--Torex introduces the XD9704/XD9705 series, compact 36V/600mA automotive buck DC/DC converters compliant with AEC-Q100 Grade 1....
-
El Khimji Ramdas Group elige a Rimini Street para reducir los costos de soporte de SAP, proteger más de 700 personalizaciones y reinvertir los ahorros en innovación
LAS VEGAS--(BUSINESS WIRE)--Rimini Street, Inc. (Nasdaq: RMNI), Software Support and Agentic AI ERP Company™ y proveedor líder de soporte de terceros para software de Oracle, SAP y VMware, anunció hoy que Khimji Ramdas Group, uno de los conglomerados privados más grandes de Omán, ha seleccionado Rimini Support™ for SAP, una medida que ha ayudado a la organización a reducir costos, reinvertir los ahorros en innovación en IA y mantener su entorno SAP ECC 6 altamente personalizado sin tiempo de in...

-
Broadstone Net Lease, Inc. Announces Pricing of Public Offering of Common Stock
VICTOR, N.Y.--(BUSINESS WIRE)--Broadstone Net Lease, Inc. Announces Pricing of Public Offering of Common Stock...

-
متحف teamLab Borderless في طوكيو يستقبل أكثر من 4 ملايين زائر من أكثر من 185 دولة حول العالم
طوكيو--(BUSINESS WIRE)--teamLab Borderless in Tokyo Welcomes Over 4 Million Visitors from more than 185 Countries...

-
Riassunto: teamLab Borderless a Tokyo accoglie oltre 4 milioni di visitatori provenienti da oltre 185 Paesi
TOKYO--(BUSINESS WIRE)--teamLab Borderless: MORI Building DIGITAL ART MUSEUM (teamLab Borderless) a Tokyo ha accolto oltre 4 milioni di visitatori al 31 luglio 2026, a circa 2 anni e 5 mesi dall'inaugurazione.*1 Questi visitatori sono arrivati da oltre 185 Paesi e regioni. I visitatori internazionali rappresentano circa il 70% del numero totale. Molti di questi visitatori internazionali provengono da Paesi e regioni lontani, tra cui Stati Uniti, Australia, Canada, Regno Unito e Germania. Il tes...

-
Purina تصبح أول عميل مؤسس لبرنامج ConnectAI Charter من NIQ يُكشف عنه رسميًا للعامة
شيكاغو--(BUSINESS WIRE)--أعلنت NielsenIQ (المدرجة في بورصة نيويورك بالرمز: NIQ)، الرائدة عالميًا في مجال ذكاء المستهلك، اليوم اختيار Purina كأول عميل يُعلن عنه رسميًا ضمن برنامج ConnectAI Charter الخاص بها. ويأتي هذا الإعلان في أعقاب إطلاق NIQ برنامجها بالتعاون مع خمس مؤسسات عالمية تمثل قطاعات العناية الشخصية، ورعاية الحيوانات الأليفة، والجمال، والمشروبات، على أن يُكشف تباعًا عن عملاء إضافيين وتُنشر دراسات حالة جديدة مع تقدم هذه الشراكات وتوسعها.من خلال ConnectAI، يعمل مهندسو NIQ المتخصصون الميد...
-
China’s Commerce Innovation Is Reshaping Global Retail
SINGAPORE--(BUSINESS WIRE)--Commerce models pioneered in China—including live commerce, social commerce and quick commerce—are increasingly influencing how consumers discover, shop and engage with brands around the world, according to latest report from NIQ (NYSE:NIQ), The Commerce Revolution: Where East Meets West. The report highlights the scale of this transformation: China’s live-commerce market reached approximately US$900 billion in 2025, approaching the size of the entire U.S. e-commerce...
-
teamLab Borderless em Tóquio recebe mais de 4 milhões de visitantes de mais de 185 países
TÓQUIO--(BUSINESS WIRE)--O teamLab Borderless: MORI Building DIGITAL ART MUSEUM (teamLab Borderless) em Tóquio recebeu mais de 4 milhões de visitantes até 31 de julho de 2026, aproximadamente 2 anos e 5 meses desde a sua abertura.*1 Esses visitantes vieram de mais de 185 países e regiões. Os visitantes internacionais correspondem a aproximadamente 70% do número total. Muitos desses visitantes internacionais vêm de países e regiões distantes, incluindo Estados Unidos, Austrália, Canadá, Reino Un...

-
Cleverbridge stärkt Wachstumsdienstleistungen durch Influencer-Marketing für Softwaremarken
KÖLN, Deutschland und CHICAGO--(BUSINESS WIRE)--Cleverbridge, ein globaler Vertriebs- und E-Commerce-Partner für Softwareunternehmen und SaaS-Anbieter, gab heute ein neues Influencer-Marketing-Angebot bekannt, das entwickelt wurde, um Kunden beim Aufbau vertrauenswürdiger Creator-Partnerschaften im Rahmen einer breit angelegten Strategie zur Nachfragegenerierung zu unterstützen. Mithilfe der Creator- und Influencer-Marketing-Plattform Later wird das Paket an Wachstumsdienstleistungen von Clever...
-
Samenvatting: teamLab Borderless in Tokio verwelkomt meer dan 4 miljoen bezoekers uit meer dan 185 landen
TOKIO--(BUSINESS WIRE)--teamLab Borderless: MORI Building DIGITAL ART MUSEUM (teamLab Borderless) in Tokio heeft per 31 juli 2026, ongeveer 2 jaar en 5 maanden na de opening, meer dan 4 miljoen bezoekers verwelkomd.*1 Deze bezoekers kwamen uit meer dan 185 landen en regio’s. Internationale bezoekers maken ongeveer 70% van het totale aantal uit. Veel van deze internationale bezoekers reizen vanuit verre landen en regio’s, waaronder de Verenigde Staten, Australië, Canada, het Verenigd Koninkrijk...
