

Newsroom
Sorted by: Latest
-
Samenvatting: Transition Industries en het Mexicaanse CFEnergía ondertekenen contract om aardgas te leveren voor de bouw van Pacifico Mexinol, 's werelds grootste ultralage-koolstofmethanolfabriek
MEXICO CITY--(BUSINESS WIRE)--Transition Industries LLC, een ontwikkelaar van wereldwijde, koolstofneutrale methanol- en waterstofprojecten, en CFEnergía, een dochteronderneming van de Mexicaanse Federale Elektriciteitscommissie (CFE), hebben bekendgemaakt dat ze een langlopend contract hebben getekend om aardgas te leveren aan het project Pacifico Mexinol (“Mexinol”) in de buurt van Topolobampo, Sinaloa. Deze bekendmaking is officieel geldend in de originele brontaal. Vertalingen zijn slechts...
-
GrayRobinson Expands Fort Myers Office with Team of Litigators
FORT MYERS, Fla.--(BUSINESS WIRE)--GrayRobinson is pleased to announce the expansion of its Fort Myers office with the addition of a seasoned team of attorneys joining the firm’s Litigation Section, including Jack C. Morgan III, Scott Hertz, John B. Gallagher, and Morgan E. Williamson. “We are thrilled to welcome Jack, Scott, John, and Morgan to GrayRobinson,” said GrayRobinson President and CEO Dean Cannon. “Their addition enhances our Fort Myers office and supports our ongoing efforts to prov...
-
Alaska Communications and SurePath AI Bring Robust GenAI Governance Capabilities with an Industry-Leading Focus on Safety and Security
ANCHORAGE, Alaska--(BUSINESS WIRE)--As generative artificial intelligence (GenAI) increasingly becomes an essential tool for businesses and enterprises, so does the need for safeguards around data security and protection. Alaska Communications is introducing Alaska businesses to a secure, enterprise‑grade path to GenAI adoption through its relationship with SurePath AI. “GenAI has become essential for organizations because of its ability to accelerate problem‑solving, increase productivity and...

-
MarketVector Indexes™ Completes Launch of U.S. Large-Cap Sector Index Family
FRANKFURT, Germany--(BUSINESS WIRE)--MarketVector Indexes™ (“MarketVector”), a global index provider specializing in thematic and digital asset benchmarks, has completed the launch of its U.S. large-cap sector index family, extending the MarketVector™ Top 500 US Profitable Companies Index into a full suite of 11 sector benchmarks. The sector indexes are designed to serve as core building blocks for U.S. equity portfolios, offering transparent, float-adjusted market-capitalization representation...

-
Retool’s 2026 Build vs. Buy Report Reveals 35% of Enterprises Have Already Replaced SaaS With Custom Software
SAN FRANCISCO--(BUSINESS WIRE)--Retool, the leading enterprise AppGen platform, today released its 2026 report ‘The Build vs. Buy Shift: How Vibe Coding and Shadow IT Have Reshaped Enterprise Software,’ which finds that enterprises are actively replacing SaaS tools with custom-built software and increasingly doing so outside traditional enterprise guardrails. Teams are replacing SaaS with custom software, with most investing more in custom tools in 2026. Many builders are also creating software...
-
Ellavoz Children’s Literacy Program Visits Oliver Street Elementary School in Newark, New Jersey
NEWARK, N.J.--(BUSINESS WIRE)--The Ellavoz Children’s Literacy Foundation (ECLF) announced today the successful visit by New York Times bestselling author, Beth Ferry, to the Oliver Street Elementary School as part of a grant program to promote literacy and encourage the love of reading. Mrs. Ferry spoke to approximately six hundred students in Kindergarten through 5th grade. Ferry, an award-winning author with over forty titles in print, took the students through the process of writing a book,...
-
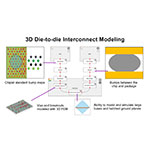
Keysight Unveils 3D Interconnect Designer for Chiplet and 3DIC Advanced Package Designs
SANTA ROSA, Calif.--(BUSINESS WIRE)--Solution addresses design bottleneck by automating complex workflows....
-
Ohana Development lance « Manchester City Yas Residences by Ohana » à Abou Dabi, un projet qui vaut 4,1 milliards USD
ABOU DABI, Émirats arabes unis--(BUSINESS WIRE)--Ohana Development, promoteur immobilier de premier plan aux Émirats arabes unis, a officiellement lancé « Manchester City Yas Residences by Ohana », un complexe résidentiel privé en bord de canal à Abou Dabi, d'une valeur de 4,1 milliards USD. Il s'agit du premier projet résidentiel de marque du Manchester City F.C. au monde. Le lancement a eu lieu à l'Etihad Park d'Abou Dabi, en présence de Husein Salem, PDG, et de Mustafa El Sammak, directeur d...

-
Celebrating 20 Years of Impact: Corvias Foundation Unveils College Connection Website
WARWICK, R.I.--(BUSINESS WIRE)--Military-connected students now have a powerful new ally in planning their academic future. Continuing its 20th anniversary celebration, Corvias Foundation, a nonprofit committed to the educational success of military-connected families and students, has launched College Connection, a free resource to help military-connected students navigate the college landscape. This launch builds on two decades of impact, including more than $20 million in scholarships awarde...

-
Efinix Announces Boon Chye (BC) Ooi Joining Board of Directors
CUPERTINO, Calif.--(BUSINESS WIRE)--Efinix®, Inc., the FPGA pioneer accelerating edge AI innovation, today announced that Boon Chye (BC) Ooi has joined its Board of Directors. Ooi, a semiconductor industry veteran with more than 45 years of operational leadership experience, will provide strategic guidance as Efinix scales its business and expands its market presence in FPGA and edge AI applications. Ooi brings unparalleled expertise in building and managing global semiconductor supply chains....