

Newsroom
Sorted by: Latest
-
Singapur beauftragt Thales mit KI-gestütztem Flugverkehrsmanagementsystem der nächsten Generation für einen der verkehrsreichsten Lufträume Asiens
MEUDON, Frankreich--(BUSINESS WIRE)--Die Zivilluftfahrtbehörde von Singapur (CAAS) hat Thales einen bedeutenden Auftrag zur Entwicklung eines neuen NexGen-Flugverkehrsmanagementsystems (ATMS) und von Flugsicherungsradaren erteilt – ein wichtiger Schritt hin zu einem effizienteren, sichereren und nachhaltigeren Luftfahrtökosystem. Das NexGen-ATMS wird das derzeitige LORADS III-System durch die Lösung TopSky – ATC One von Thales ablösen. Das Projekt sieht außerdem einen umfassenden Wissenstransfe...

-
RHI Magnesita 2026 Half Year Results: Consistent Self-help Delivery and Strong Steel Business Performance Delivers 42% Adj. EBITA Growth on Constant Currency Basis
VIENNA--(BUSINESS WIRE)--RHI Magnesita, the leading global supplier of high-grade refractory products, systems and solutions, announces its results for the six months ended 30 June 2026. Strong earnings improvement despite continued market weakness RHI Magnesita delivered a solid earnings improvement in the first half of 2026, supported by continued execution of management-led self-help measures and strong performance in the Steel segment. Adjusted EBITA increased by €24 million, or 17%, to €16...

-
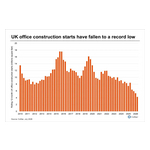
CoStar Data Shows London Dominates UK Office Development as Regional Pipeline Hits 20-Year Low
LONDON--(BUSINESS WIRE)--Office construction in UK regions has fallen to its lowest level in at least 20 years, according to data from CoStar, a global leading provider of online real estate marketplaces, information and analytics in the property markets. Preliminary data for Q2 2026 shows annual office construction starts fell below 5 million square feet for the first time since at least 2010, far below the 16 million square feet recorded in 2019, when conditions were more supportive. “The fal...
-
Mitsubishi Electric Announces Consolidated Financial Results for the First Quarter of Fiscal 2027
TOKYO--(BUSINESS WIRE)--Mitsubishi Electric Corporation (TOKYO: 6503) announced today its consolidated financial results for the first quarter, ended June 30, 2026, of the current fiscal year ending March 31, 2027 (fiscal 2027). The full document on Mitsubishi Electric’s financial results can be viewed at the following link: www.MitsubishiElectric.com/en/pr Consolidated Financial Results Billions of yen Q1 FY26 Q1 FY27 YoY Revenue 1,312.8 1,497.1 +184.2 114% Adjusted operating profit 93.8 144.3...
-
Orano: Résultats semestriels 2026 en ligne avec les perspectives annuelles malgré des arrêts de production conjoncturels
PARIS--(BUSINESS WIRE)--Regulatory News: Orano: Activité globalement stable avec des situations contrastées par secteur, EBITDA pénalisé par des arrêts de production Chiffre d’affaires de 2 696 M€, en légère progression de + 2,1 % (p.c.c.), marqué par une bonne performance du secteur Aval et un écoulement moins favorable du carnet de commandes des secteurs Mines et Amont entre les deux périodes. EBITDA en baisse à 595 M€ (contre 727 M€ au 1er semestre 2025) compte tenu d’arrêts de production da...
-
Orano: 2026 Half-Year Results in Line With Annual Outlook Despite Circumstantial Production Stoppages
PARIS--(BUSINESS WIRE)--Orano: 2026 half-year results in line with annual outlook despite circumstantial production stoppages...
-
Renesas Reports Financial Results for the Second Quarter Ended June 30, 2026
TOKYO--(BUSINESS WIRE)--Renesas announced consolidated financial results in accordance with IFRS for the three and six months ended June 30, 2026....

-
Renesas to Phase Out Production at Takasaki Factory; Maintain and Strengthen R&D Functions
TOKYO--(BUSINESS WIRE)--Renesas will gradually scale down and end manufacturing operations at the Takasaki Factory over the next 2 to 3 years while maintaining R&D functions....

-
Polpharma Biologics Announces FDA and EMA Acceptance for Review of PB016 Vedolizumab Biosimilar Candidate
ROTKREUZ, Switzerland--(BUSINESS WIRE)--Polpharma Biologics International AG today announces that the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have accepted for review the Biologics License Application (BLA) and Marketing Authorisation Application (MAA), respectively, for PB016, a proposed vedolizumab biosimilar candidate to Takeda’s reference product Entyvio®* (vedolizumab) lyophilized vial for intravenous (IV) administration for the treatment of adults w...

-
Renesas Announces Consolidated Forecasts
TOKYO--(BUSINESS WIRE)--Renesas today announced the consolidated financial forecasts for the nine months ending September 30, 2026....
