

Newsroom
Sorted by: Latest
-
First Trust Global Funds PLC UK Regulatory Announcement: Net Asset Value(s)
LONDON--(BUSINESS WIRE)-- Funds Date TIDM ISIN Code Shares in Issue Currency Net Asset Value NAV/per Share First Trust Alerian Disruptive Technology Real Estate UCITS ETF 20.03.2026 LANDXN.LN IE000RN036E0 34,035.00 USD 687,997.24 20.214 ...
-
Sudden Cardiac Death Risk and Heart Failure Management at ACC.26 – How ZOLL Innovations Redefine Protection
CHELMSFORD, Mass.--(BUSINESS WIRE)--ZOLL®, an Asahi Kasei company that manufactures medical devices and related software solutions, will highlight the latest sudden cardiac death research, case experiences for heart failure readmission reduction, and two Innovation Stage presentations at the American College of Cardiology Annual Scientific Session & Expo (ACC.26), March 28-30, 2026. ZOLL will sponsor a slate of educational programs to engage and connect clinicians with emerging evidence and...
-
Polymarket Publishes Enhanced Market Integrity Rules Across Its DeFi Platform and CFTC-Regulated U.S. Exchange
NEW YORK--(BUSINESS WIRE)--Polymarket, the world’s largest prediction market, today announced updated market integrity rules across both its DeFi platform and its CFTC-regulated U.S. exchange. The rules, which appear in the DeFi platform’s Terms of Use and the Polymarket US Rulebook, amplify Polymarket’s requirements governing insider trading and market manipulation and reinforce Polymarket’s commitment to maintaining the quality of its markets and protecting its users. "Markets thrive on clari...
-
Yubico Expands Enrollment Services to Accelerate Enterprises to Phishing-resistance and Passwordless
SAN FRANCISCO--(BUSINESS WIRE)--Regulatory News Yubico (NASDAQ STOCKHOLM: YUBICO), a cybersecurity company and creator of the YubiKey, the most secure passkey, today at RSA Conference announced the expansion of its Enrollment services – available exclusively through YubiKey as a Service – to include support for simple and secure in-the-field enrollment of YubiKeys for Microsoft and PingID environments. These expanded enrollment options help customers fast track to phishing-resistance and passwo...
-
Houlihan Lokey Strengthens Capital Solutions Group With Senior Real Estate Hire
NEW YORK--(BUSINESS WIRE)--Houlihan Lokey, Inc. (NYSE:HLI), the global investment bank, announced today that Steven Loffman has joined as a Managing Director in its Capital Solutions Group. Mr. Loffman will be based in New York and will lead the U.S. Real Estate Capital Advisory practice for the firm. This announcement follows the firm’s recent addition of Mellum Capital, a European based real estate capital advisory business bringing the firm’s global real estate capital solutions practice to...

-
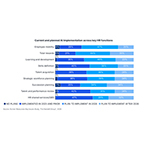
The Hackett Group®: HR Leaders Ramp Up AI Investment as Pressure to Evolve Intensifies
MIAMI--(BUSINESS WIRE)--The Hackett Group, Inc. (NASDAQ: HCKT), a leading Gen AI consultancy and enterprise digital transformation firm, today announced findings from its 2026 Human Resources Key Issues Study. The research shows that human resources (HR) leaders broadly recognize the need to transform, but execution remains uneven – creating a widening disconnect between strategic priorities and day-to-day activities as workforce demands intensify. The numbers tell a clear story: HR workloads a...
-
Ateios Systems and Kodak Expand RaiCore™ Platform to Major Battery Chemistries and Earn PFAS-Free Verification
NEWBERRY, Ind.--(BUSINESS WIRE)--Ateios Systems and Kodak Expand RaiCoreTM Platform to Major Battery Chemistries and Earn PFAS-Free Verification...
-
Dell Technologies Expands Cybersecurity and Resilience for the AI Era and Emerging Quantum Risks
SAN FRANCISCO--(BUSINESS WIRE)--Dell Technologies (NYSE: DELL) introduces new security by design and cyber resilience capabilities to help organizations secure, detect and recover from next-generation threats. The enhancements address emerging risks from quantum computing and AI by hardening device foundations, strengthening cyber resilience when incidents occur and extending threat detection into AI data platforms. Why it matters AI is creating more valuable data and giving attackers new ways...
-
Tsunami Express Car Wash Becomes Partner and Official Car Wash of the Milwaukee Brewers™
MILWAUKEE--(BUSINESS WIRE)--Tsunami Express Car Wash is thrilled to announce an exciting new partnership as the Official Car Wash of the Milwaukee Brewers™, bringing together two brands with deep roots in Wisconsin communities and a shared commitment to delivering exceptional experiences. Tsunami Express Car Wash is one of the Midwest’s fastest-growing car wash brands, with a particularly strong presence in Wisconsin. The company operates 16 locations across the state, including 11 in the Great...
-
Toshiba Showcases Advanced Power Semiconductor Solutions at APEC 2026
IRVINE, Calif.--(BUSINESS WIRE)--Toshiba showcases advanced power semiconductor solutions at APEC 2026....
