

Newsroom
Sorted by: Latest
-
Rosen Law Firm Urges Avis Budget Group, Inc. (NASDAQ: CAR) Stockholders to Contact the Firm for Information About Their Rights
NEW YORK--(BUSINESS WIRE)--Rosen Law Firm, a global investor rights law firm, announces a class action lawsuit on behalf of purchasers of securities of Avis Budget Group, Inc. (NASDAQ: CAR), including those who bought Avis common stock to cover a short position, between February 20, 2025 and April 21, 2026, inclusive (the “Class Period”).For more information, submit a form, email attorney Phillip Kim, or give us a call at 866-767-3653.The Allegations: Rosen Law Firm is Investigating the Allegati...
-
Paycom Announces Quarterly Cash Dividend
OKLAHOMA CITY--(BUSINESS WIRE)--Paycom Software, Inc. (“Paycom”) (NYSE: PAYC), a leading provider of comprehensive, cloud-based human capital management software, announced today that its Board of Directors declared a cash dividend in the amount of $0.375 per share of common stock, to be paid on Sept. 8, 2026, to all stockholders of record as of the close of business on Aug. 24, 2026. About Paycom Paycom Software, Inc. (NYSE: PAYC) is a cloud-based human capital management software provider tha...
-
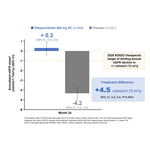
Otsuka Unveils Unprecedented Phase 3 VISIONARY Two-Year eGFR Results Demonstrating VOYXACT® (sibeprenlimab-szsi) Stabilizes Kidney Function Decline to Baseline Physiologic Rate, Fundamentally Altering Disease Progression in IgA Nephropathy (IgAN)
PRINCETON, N.J. & TOKYO--(BUSINESS WIRE)--Otsuka Pharmaceutical Development & Commercialization, Inc. and Otsuka Pharmaceutical Co., Ltd. (Otsuka) announced new data from the Phase 3 VISIONARY trial demonstrating that VOYXACT® (sibeprenlimab-szsi) stabilizes estimated glomerular filtration rate (eGFR) returning kidney function decline to baseline physiologic rate over two years (24 months) in adults with primary IgA nephropathy (IgAN) at risk for disease progression. Results presented durin...
-
Black Stone Minerals, L.P. Reports Second Quarter Results
HOUSTON--(BUSINESS WIRE)--Black Stone Minerals, L.P. (NYSE: BSM) ("Black Stone Minerals," "Black Stone," or "the Partnership") today announces its financial and operating results for the second quarter of 2026. Financial and Operational Highlights Net income for the second quarter was $106.4 million, and Adjusted EBITDA for the quarter totaled $91.3 million. Distributable cash flow was $80.4 million for the second quarter. Mineral and royalty production for the second quarter of 2026 equaled 32...
-
Northern Trust Announces Redemption of Series D Preferred Stock
CHICAGO--(BUSINESS WIRE)--Northern Trust Corp. today announced the redemption on October 1, of all outstanding shares of its Series D Non-Cumulative Perpetual Preferred Stock....

-
N-able to Host Second Quarter Earnings Conference Call on August 10, 2026
BURLINGTON, Mass.--(BUSINESS WIRE)--N-able, Inc. (NYSE:NABL), a global cybersecurity company delivering business resilience, today announced that it will host a conference call to discuss its financial results for the second quarter of 2026 at 8:30 a.m. ET on August 10, 2026. A live webcast of the call will be available on the N-able Investor Relations website at http://investors.n-able.com. A replay of the webcast will be available on a temporary basis shortly after the event. N-able will issu...
-
Citizens Financial Group, Inc. Declares Dividends on Preferred Stock
PROVIDENCE, R.I.--(BUSINESS WIRE)--Citizens Financial Group, Inc. (NYSE: CFG) announced that its board of directors has declared the following dividends on its preferred stock payable on October 6, 2026, to preferred shareholders of record at the close of business on September 21, 2026: a quarterly cash dividend of $17.93138778 per share on CFG’s 6.000% Fixed-to-Floating Rate Non-Cumulative Perpetual Preferred Stock, Series B (CUSIP No. 174610AP0); a quarterly cash dividend of $18.32494333 per...
-
CAPR Class Action Lawsuit FILED: Capricor Therapeutics Sued for Securities Fraud after Stock Drops 64% Leading to Securities Fraud Case – Investors Urged to Contact BFA Law
NEW YORK--(BUSINESS WIRE)--Capricor Therapeutics Sued for Securities Fraud after Stock Drops 64% Leading to Securities Fraud Case – Investors Urged to Contact BFA Law...
-
Better Home & Finance Appoints Daniel Lewis Interim Chief Executive Officer
NEW YORK--(BUSINESS WIRE)--Better Home & Finance Holding Company (NASDAQ: BETR) (“Better” or the “Company”), the leading AI-native homeownership company, today announced that the Company’s Board of Directors (the “Board”) has appointed Board member, Daniel Lewis, Interim Chief Executive Officer, effective immediately. Mr. Lewis succeeds Founder Vishal Garg, who has mutually agreed with the Board to transition from his role as Chief Executive Officer. Mr. Garg will continue to serve on the B...
-
Innovative Industrial Properties Reports Second Quarter 2026 Results
SAN DIEGO--(BUSINESS WIRE)--Innovative Industrial Properties, Inc. (NYSE: IIPR) ("IIP" or the "Company") announced today results for the second quarter ended June 30, 2026. Executive Chairman Remarks “Our second quarter activity reflects the continued execution of our strategy across multiple fronts by our management team. We completed the funding of our $270 million investment in IQHQ, generated meaningful leasing momentum across our portfolio and proactively strengthened our balance sheet thr...